What Is Calcaneal Apophysitis?
Overview
Sever's disease is a condition characterized by pain in one or both heels with walking. The pain is caused by shortening of the heel-cord. It usually affects children between the ages of 10 and 13 years old. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Sever's disease is also called calcaneal apophysitis.
Causes
Sever's Disease is a repetitive strain injury caused by the following. High impact injury activities and sport like netball, football, soccer, hockey, basketball, running, jumping and tennis. Tight calf muscles. Poor mechanics, structure and function of the foot. Excessive pronation. Rapid growth spurt. The above causes tension, inflammation and pain where the Achilles tendon inserts onto the calcaneus (Back/bottom surface of the heel bone). It is important that this problem is treated and monitored until the growth plate ossifies in the heel. This could occur between the ages of 14 and 16 years of age. In extreme cases the growth plate can become separated from the calcaneus.
Symptoms
The symptoms of Sever?s Disease may vary but usually include generalised pain and discomfort around the back of the heel. Can be one sided or both sides. Starts after child starts a new sport season. May cause child to limp due to pain. Increases with weight bearing activity. Heel becomes red and can be swollen. X-rays are usually inconclusive and simply show the growth plate.
Diagnosis
The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
Stretching programs. Strengthening exercises. Exercise and training modification. Orthotic therapy. In rare cases, where fragmentation of the apophysis exists and pain fails to subside with traditional treatments then immobilization of the foot and ankle with a short leg pneumatic walker(walking cast) is indicated.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Sever's disease is a condition characterized by pain in one or both heels with walking. The pain is caused by shortening of the heel-cord. It usually affects children between the ages of 10 and 13 years old. During this phase of life, growth of the bone is taking place at a faster rate than the tendons. Sever's disease is also called calcaneal apophysitis.
Causes
Sever's Disease is a repetitive strain injury caused by the following. High impact injury activities and sport like netball, football, soccer, hockey, basketball, running, jumping and tennis. Tight calf muscles. Poor mechanics, structure and function of the foot. Excessive pronation. Rapid growth spurt. The above causes tension, inflammation and pain where the Achilles tendon inserts onto the calcaneus (Back/bottom surface of the heel bone). It is important that this problem is treated and monitored until the growth plate ossifies in the heel. This could occur between the ages of 14 and 16 years of age. In extreme cases the growth plate can become separated from the calcaneus.
Symptoms
The symptoms of Sever?s Disease may vary but usually include generalised pain and discomfort around the back of the heel. Can be one sided or both sides. Starts after child starts a new sport season. May cause child to limp due to pain. Increases with weight bearing activity. Heel becomes red and can be swollen. X-rays are usually inconclusive and simply show the growth plate.
Diagnosis
The doctor may order an x-ray because x-rays can confirm how mature the growth center is and if there are other sources of heel pain, such as a stress fracture or bone cyst. However, x-rays are not necessary to diagnose Sever?s disease, and it is not possible to make the diagnosis based on the x-ray alone.
Non Surgical Treatment
Stretching programs. Strengthening exercises. Exercise and training modification. Orthotic therapy. In rare cases, where fragmentation of the apophysis exists and pain fails to subside with traditional treatments then immobilization of the foot and ankle with a short leg pneumatic walker(walking cast) is indicated.
Surgical Treatment
The surgeon may select one or more of the following options to treat calcaneal apophysitis. Reduce activity. The child needs to reduce or stop any activity that causes pain. Support the heel. Temporary shoe inserts or custom orthotic devices may provide support for the heel. Medications. Nonsteroidal anti-inflammatory drugs (NSAIDs), such as ibuprofen, help reduce the pain and inflammation. Physical therapy. Stretching or physical therapy modalities are sometimes used to promote healing of the inflamed issue. Immobilization. In some severe cases of pediatric heel pain, a cast may be used to promote healing while keeping the foot and ankle totally immobile. Often heel pain in children returns after it has been treated because the heel bone is still growing. Recurrence of heel pain may be a sign of calcaneal apophysitis, or it may indicate a different problem. If your child has a repeat bout of heel pain, be sure to make an appointment with your foot and ankle surgeon.
Posterior Tibial Tendon Dysfunction Physical Therapy
Overview
Originally known as posterior tibial tendon dysfunction or insufficiency, adult-acquired flatfoot deformity encompasses a wide range of deformities. These deformities vary in location, severity, and rate of progression. Establishing a diagnosis as early as possible is one of the most important factors in treatment. Prompt early, aggressive nonsurgical management is important. A patient in whom such treatment fails should strongly consider surgical correction to avoid worsening of the deformity. In all four stages of deformity, the goal of surgery is to achieve proper alignment and maintain as much flexibility as possible in the foot and ankle complex. However, controversy remains as to how to manage flexible deformities, especially those that are severe. 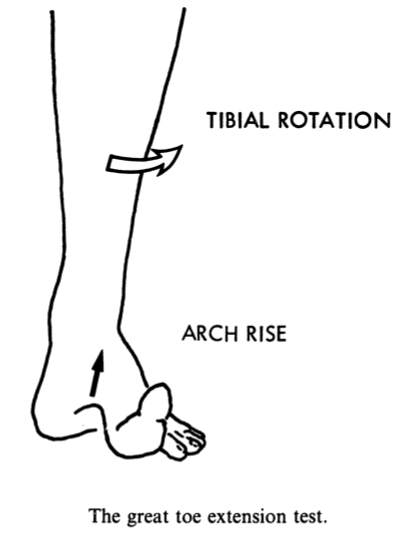
Causes
Causes of an adult acquired flatfoot may include Neuropathic foot (Charcot foot) secondary to Diabetes mellitus, Leprosy, Profound peripheral neuritis of any cause. Degenerative changes in the ankle, talonavicular or tarsometatarsal joints, or both, secondary to Inflammatory arthropathy, Osteoarthropathy, Fractures, Acquired flatfoot resulting from loss of the supporting structures of the medial longitudinal arch. Dysfunction of the tibialis posterior tendon Tear of the spring (calcaneoanvicular) ligament (rare). Tibialis anterior rupture (rare). Painful flatfoot can have other causes, such as tarsal coalition, but as such a patient will not present with a change in the shape of the foot these are not included here.
Symptoms
Pain along the inside of the foot and ankle, where the tendon lies. This may or may not be associated with swelling in the area. Pain that is worse with activity. High-intensity or high-impact activities, such as running, can be very difficult. Some patients can have trouble walking or standing for a long time. Pain on the outside of the ankle. When the foot collapses, the heel bone may shift to a new position outwards. This can put pressure on the outside ankle bone. The same type of pain is found in arthritis in the back of the foot. Asymmetrical collapsing of the medial arch on the affected side.
Diagnosis
Starting from the knee down, check for any bowing of the tibia. A tibial varum will cause increased medial stress on the foot and ankle. This is essential to consider in surgical planning. Check the gastrocnemius muscle and Achilles complex via a straight and bent knee check for equinus. If the range of motion improves to at least neutral with bent knee testing of the Achilles complex, one may consider a gastrocnemius recession. If the Achilles complex is still tight with bent knee testing, an Achilles lengthening may be necessary. Check the posterior tibial muscle along its entire course. Palpate the muscle and observe the tendon for strength with a plantarflexion and inversion stress test. Check the flexor muscles for strength in order to see if an adequate transfer tendon is available. Check the anterior tibial tendon for size and strength.
Non surgical Treatment
In the early stages, simple pre-fabricated orthotics can help improve the heel position to reduce the mechanical load which is contributing to the symptoms. In advanced stages or long term orthotic use, a plaster of paris or foam box cast can be taken and specific bespoke orthotics manufactured. If the condition develops further a AFO (ankle foot orthotic) may be necessary for greater control. In more advanced stages of symptomatic Adult Acquired flat feet, where the conservative methods of treatment have failed there are various forms of surgery available depending upon the root cause of the issue and severity. 
Surgical Treatment
The indications for surgery are persistent pain and/or significant deformity. Sometimes the foot just feels weak and the assessment of deformity is best done by a foot and ankle specialist. If surgery is appropriate, a combination of soft tissue and bony procedures may be considered to correct alignment and support the medial arch, taking strain off failing ligaments. Depending upon the tissues involved and extent of deformity, the foot and ankle specialist will determine the necessary combination of procedures. Surgical procedures may include a medial slide calcaneal osteotomy to correct position of the heel, a lateral column lengthening to correct position in the midfoot and a medial cuneiform osteotomy or first metatarsal-tarsal fusion to correct elevation of the medial forefoot. The posterior tibial tendon may be reconstructed with a tendon transfer. In severe cases (stage III), the reconstruction may include fusion of the hind foot,, resulting in stiffness of the hind foot but the desired pain relief. In the most severe stage (stage IV), the deltoid ligament on the inside of the ankle fails, resulting in the deformity in the ankle. This deformity over time can result in arthritis in the ankle.
Do You Understand Heel Soreness?
Overview

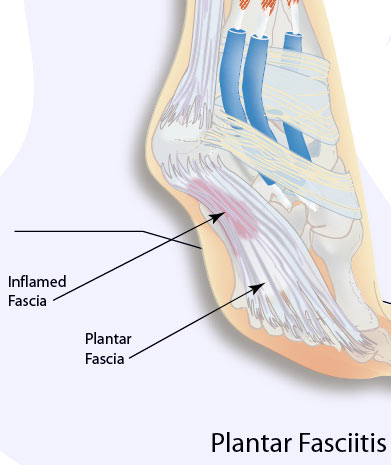
Pain arises in the centre of the heel and sometimes can spread to the arch region of the foot. Some patients complain of intense Heel Pain when walking the first few steps in the morning and after periods of rest. The most common cause of heel pain is plantar fascitis. The plantar fascia is a broad band of tissue that runs along the bottom of the foot. When this band of tissue is damaged due to biomechanical reasons or inappropriate running shoes then the tissue can become inflamed or even tear at the heel bone. This can be very painful.
Causes
As stated above, if biomechanical complaints such as over pronation exist during running then this can lead to planter fascitis and heel pain. Over pronation occurs when there is excessive mobility in the sab-taler joint of the foot which causes hyper mobility of the foot. Conditions such as flat feet can also cause over pronation. This increased mobility adversely affects all the muscles in the foot and can even affect the lower leg, upper leg and cause back pain. The mechanical imbalance is highlighted during running due to the increased forces being applied to the body Runners often complain that the pain increases when they enter the toe off phase of the running cycle as this stretches the muscle away from the heel bone. Apart from over pronation, other causes of planter fascitis are a change of running shoes, dramatic increases in speed work, hill work and mileage.
Symptoms
Symptoms may also include swelling that is quite tender to the touch. Standing, walking and constrictive shoe wear typically aggravate symptoms. Many patients with this problem are middle-aged and may be slightly overweight. Another group of patients who suffer from this condition are young, active runners.
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
Treatment for plantar fasciitis should be directed at resting the plantar fascia, providing support for the arch area and limiting pronation. This is often accomplished with the use of supportive strapping with athletic tape, arch supports and orthotics. Heel lifts may also be helpful. Anti-inflammatories, pills as well as cortisone injections, may be effective as an adjunctive treatment by speeding up the reduction of inflammation. However, if used alone, anti-inflammatories rarely lead to resolution of the condition. Stretching exercises, physical therapy and night splints may also be helpful. The majority of cases respond to non-surgical treatment although it may take several weeks to reach a comfortable level. In those cases that do not respond adequately to conservative measures, surgical release of the plantar fascia may be considered. However, a new non-surgical treatment called Extracorporeal Shockwave Therapy (ESWT) is now available as an option for recalcitrant plantar fasciitis. ESWT was approved by the FDA recently for the treatment of chronic heel pain. It has been in use for several years on thousands of patients in Europe and has been successfully used to restore patients with chronic plantar fasciitis to a normal, active lifestyle. ESWT is a non-invasive procedure that uses high intensity sound waves similar to what is routinely used to treat kidney stones. The treatment is usually performed in the office or in an outpatient surgical center. The procedure is performed under local anesthesia and takes about 25 minutes. The shockwaves are directed at the plantar fascia and stimulate an inflammatory healing response.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
Prevention

You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
Pain arises in the centre of the heel and sometimes can spread to the arch region of the foot. Some patients complain of intense Heel Pain when walking the first few steps in the morning and after periods of rest. The most common cause of heel pain is plantar fascitis. The plantar fascia is a broad band of tissue that runs along the bottom of the foot. When this band of tissue is damaged due to biomechanical reasons or inappropriate running shoes then the tissue can become inflamed or even tear at the heel bone. This can be very painful.
Causes
As stated above, if biomechanical complaints such as over pronation exist during running then this can lead to planter fascitis and heel pain. Over pronation occurs when there is excessive mobility in the sab-taler joint of the foot which causes hyper mobility of the foot. Conditions such as flat feet can also cause over pronation. This increased mobility adversely affects all the muscles in the foot and can even affect the lower leg, upper leg and cause back pain. The mechanical imbalance is highlighted during running due to the increased forces being applied to the body Runners often complain that the pain increases when they enter the toe off phase of the running cycle as this stretches the muscle away from the heel bone. Apart from over pronation, other causes of planter fascitis are a change of running shoes, dramatic increases in speed work, hill work and mileage.
Symptoms
Symptoms may also include swelling that is quite tender to the touch. Standing, walking and constrictive shoe wear typically aggravate symptoms. Many patients with this problem are middle-aged and may be slightly overweight. Another group of patients who suffer from this condition are young, active runners.
Diagnosis
The diagnosis of plantar fasciitis is generally made during the history and physical examination. There are several conditions that can cause heel pain, and plantar fasciitis must be distinguished from these conditions. Pain can be referred to the heel and foot from other areas of the body such as the low back, hip, knee, and/or ankle. Special tests to challenge these areas are performed to help confirm the problem is truly coming from the plantar fascia. An X-ray may be ordered to rule out a stress fracture of the heel bone and to see if a bone spur is present that is large enough to cause problems. Other helpful imaging studies include bone scans, MRI, and ultrasound. Ultrasonographic exam may be favored as it is quick, less expensive, and does not expose you to radiation. Laboratory investigation may be necessary in some cases to rule out a systemic illness causing the heel pain, such as rheumatoid arthritis, Reiter's syndrome, or ankylosing spondylitis. These are diseases that affect the entire body but may show up at first as pain in the heel.
Non Surgical Treatment
Treatment for plantar fasciitis should be directed at resting the plantar fascia, providing support for the arch area and limiting pronation. This is often accomplished with the use of supportive strapping with athletic tape, arch supports and orthotics. Heel lifts may also be helpful. Anti-inflammatories, pills as well as cortisone injections, may be effective as an adjunctive treatment by speeding up the reduction of inflammation. However, if used alone, anti-inflammatories rarely lead to resolution of the condition. Stretching exercises, physical therapy and night splints may also be helpful. The majority of cases respond to non-surgical treatment although it may take several weeks to reach a comfortable level. In those cases that do not respond adequately to conservative measures, surgical release of the plantar fascia may be considered. However, a new non-surgical treatment called Extracorporeal Shockwave Therapy (ESWT) is now available as an option for recalcitrant plantar fasciitis. ESWT was approved by the FDA recently for the treatment of chronic heel pain. It has been in use for several years on thousands of patients in Europe and has been successfully used to restore patients with chronic plantar fasciitis to a normal, active lifestyle. ESWT is a non-invasive procedure that uses high intensity sound waves similar to what is routinely used to treat kidney stones. The treatment is usually performed in the office or in an outpatient surgical center. The procedure is performed under local anesthesia and takes about 25 minutes. The shockwaves are directed at the plantar fascia and stimulate an inflammatory healing response.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
Prevention
You can try to avoid the things that cause heel pain to start avoid becoming overweight, where your job allows, minimise the shock to your feet from constant pounding on hard surfaces, reduce the shocks on your heel by choosing footwear with some padding or shock-absorbing material in the heel, if you have high-arched feet or flat feet a moulded insole in your shoe may reduce the stresses on your feet, if you have an injury to your ankle or foot, make sure you exercise afterwards to get back as much movement as possible to reduce the stresses on your foot and your heel in particular, If you start to get heel pain, doing the above things may enable the natural healing process to get underway and the pain to improve.
What Is The Main Cause Of Achilles Tendinitis ?
Overview
 Achilles tendinitis is an overuse injury common in many sports that require lots of running and jumping. Once this condition becomes more chronic adhesions that form along the tissues and the injury becomes more of a tendinosis. Treatment for a tendinosis is much different that for a tendinitis, so it is important to recognize what stage the injury is at in order to treat it appropriately. An acute achilles tendinitis involves inflammation and would be treated with rest, ice, etc. Once the inflammation has decreased, research shows that eccentric exercises are beneficial. Once there is tendinosis, it becomes imperative to break up those adhesions with ART and prescribe appropriate stretches and exercises.
Achilles tendinitis is an overuse injury common in many sports that require lots of running and jumping. Once this condition becomes more chronic adhesions that form along the tissues and the injury becomes more of a tendinosis. Treatment for a tendinosis is much different that for a tendinitis, so it is important to recognize what stage the injury is at in order to treat it appropriately. An acute achilles tendinitis involves inflammation and would be treated with rest, ice, etc. Once the inflammation has decreased, research shows that eccentric exercises are beneficial. Once there is tendinosis, it becomes imperative to break up those adhesions with ART and prescribe appropriate stretches and exercises.
Causes
Over-pronation, injury and overstresses of the tendon are some of the most common causes. Risk factors include tight heel cords, poor foot alignment, and recent changes in activities or shoes. During a normal gait cycle, the upper and lower leg rotate in unison (i.e. internally during pronation and externally during supination). However, when a person over-pronates, the lower leg is locked into the foot and therefore continues to rotate internally past the end of the contact phase while the femur begins to rotate externally at the beginning of midstance. The Gastrocnemius muscle is attached to the upper leg and rotates externally while the Soleus muscle is attached to the lower leg and rotates internally during pronation. The resulting counter rotation of the upper and lower leg causes a shearing force to occur in the Achilles tendon. This counter rotation twists the tendon at its weakest area, namely the Achilles tendon itself, and causes the inflammation. Since the tendon is avascular, once inflammation sets in, it tends to be chronic.
Symptoms
Achilles tendonitis typically starts off as a dull stiffness in the tendon, which gradually goes away as the area gets warmed up. It may get worse with faster running, uphill running, or when wearing spikes and other low-heeled running shoes. If you continue to train on it, the tendon will hurt more sharply and more often, eventually impeding your ability even to jog lightly. About two-thirds of Achilles tendonitis cases occur at the ?midpoint? of the tendon, a few inches above the heel. The rest are mostly cases of ?insertional? Achilles tendonitis, which occurs within an inch or so of the heelbone. Insertional Achilles tendonitis tends to be more difficult to get rid of, often because the bursa, a small fluid-filled sac right behind the tendon, can become irritated as well.
Diagnosis
Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Imaging studies. Plain radiography: Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography: Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst; in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI): MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis.
Nonsurgical Treatment
In order to treat the symptoms, antiflogistics or other anti-inflammatory therapy are often used. However these forms of therapy usually cannot prevent the injury to live on. Nevertheless patients will always have to be encouraged to execute less burdening activities, so that the burden on the tendon decreases as well. Complete immobilisation should however be avoided, since it can cause atrophy. Passive rehabilitation, Mobilisations can be used for dorsiflexion limitation of the talocrural joint and varus- or valgus limitation of the subtalar joint. Deep cross frictions (15 min). It?s effectiveness is not scientifically proven and gives limited results. Recently, the use of Extracorporal Shock Wave Therapy was proven. Besides that, the application of ice can cause a short decrease in pain and in swelling. Even though cryotherapy 2, 5 was not studied very thoroughly, recent research has shown that for injuries of soft tissue, applications of ice through a wet towel for ten minutes are the most effective measures. Active rehabilitation, An active exercise program mostly includes eccentric exercises. This can be explained by the fact that eccentric muscle training will lengthen the muscle fibres, which stimulates the collagen production. This form of therapy appears successful for mid-portion tendinosis, but has less effect with insertion tendinopathy. The sensation of pain sets the beginning burdening of the patient and the progression of the exercises.

Surgical Treatment
Surgery is considered the last resort. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
Achilles tendinitis is an overuse injury common in many sports that require lots of running and jumping. Once this condition becomes more chronic adhesions that form along the tissues and the injury becomes more of a tendinosis. Treatment for a tendinosis is much different that for a tendinitis, so it is important to recognize what stage the injury is at in order to treat it appropriately. An acute achilles tendinitis involves inflammation and would be treated with rest, ice, etc. Once the inflammation has decreased, research shows that eccentric exercises are beneficial. Once there is tendinosis, it becomes imperative to break up those adhesions with ART and prescribe appropriate stretches and exercises.
Causes
Over-pronation, injury and overstresses of the tendon are some of the most common causes. Risk factors include tight heel cords, poor foot alignment, and recent changes in activities or shoes. During a normal gait cycle, the upper and lower leg rotate in unison (i.e. internally during pronation and externally during supination). However, when a person over-pronates, the lower leg is locked into the foot and therefore continues to rotate internally past the end of the contact phase while the femur begins to rotate externally at the beginning of midstance. The Gastrocnemius muscle is attached to the upper leg and rotates externally while the Soleus muscle is attached to the lower leg and rotates internally during pronation. The resulting counter rotation of the upper and lower leg causes a shearing force to occur in the Achilles tendon. This counter rotation twists the tendon at its weakest area, namely the Achilles tendon itself, and causes the inflammation. Since the tendon is avascular, once inflammation sets in, it tends to be chronic.
Symptoms
Achilles tendonitis typically starts off as a dull stiffness in the tendon, which gradually goes away as the area gets warmed up. It may get worse with faster running, uphill running, or when wearing spikes and other low-heeled running shoes. If you continue to train on it, the tendon will hurt more sharply and more often, eventually impeding your ability even to jog lightly. About two-thirds of Achilles tendonitis cases occur at the ?midpoint? of the tendon, a few inches above the heel. The rest are mostly cases of ?insertional? Achilles tendonitis, which occurs within an inch or so of the heelbone. Insertional Achilles tendonitis tends to be more difficult to get rid of, often because the bursa, a small fluid-filled sac right behind the tendon, can become irritated as well.
Diagnosis
Laboratory studies usually are not necessary in evaluating and diagnosing an Achilles tendon rupture or injury, although evaluation may help to rule out some of the other possibilities in the differential diagnosis. Imaging studies. Plain radiography: Radiographs are more useful for ruling out other injuries than for ruling in Achilles tendon ruptures. Ultrasonography: Ultrasonography of the leg and thigh can help to evaluate the possibility of deep venous thrombosis and also can be used to rule out a Baker cyst; in experienced hands, ultrasonography can identify a ruptured Achilles tendon or the signs of tendinosis. Magnetic resonance imaging (MRI): MRI can facilitate definitive diagnosis of a disrupted tendon and can be used to distinguish between paratenonitis, tendinosis, and bursitis.
Nonsurgical Treatment
In order to treat the symptoms, antiflogistics or other anti-inflammatory therapy are often used. However these forms of therapy usually cannot prevent the injury to live on. Nevertheless patients will always have to be encouraged to execute less burdening activities, so that the burden on the tendon decreases as well. Complete immobilisation should however be avoided, since it can cause atrophy. Passive rehabilitation, Mobilisations can be used for dorsiflexion limitation of the talocrural joint and varus- or valgus limitation of the subtalar joint. Deep cross frictions (15 min). It?s effectiveness is not scientifically proven and gives limited results. Recently, the use of Extracorporal Shock Wave Therapy was proven. Besides that, the application of ice can cause a short decrease in pain and in swelling. Even though cryotherapy 2, 5 was not studied very thoroughly, recent research has shown that for injuries of soft tissue, applications of ice through a wet towel for ten minutes are the most effective measures. Active rehabilitation, An active exercise program mostly includes eccentric exercises. This can be explained by the fact that eccentric muscle training will lengthen the muscle fibres, which stimulates the collagen production. This form of therapy appears successful for mid-portion tendinosis, but has less effect with insertion tendinopathy. The sensation of pain sets the beginning burdening of the patient and the progression of the exercises.
Surgical Treatment
Surgery is considered the last resort. It is only recommended if all other treatment options have failed after at least six months. In this situation, badly damaged portions of the tendon may be removed. If the tendon has ruptured, surgery is necessary to re-attach the tendon. Rehabilitation, including stretching and strength exercises, is started soon after the surgery. In most cases, normal activities can be resumed after about 10 weeks. Return to competitive sport for some people may be delayed for about three to six months.
Prevention
Although Achilles tendinitis cannot be completely prevented, the risk of developing it can be lowered. Being aware of the possible causes does help, but the risk can be greatly reduced by taking the following precautions. Getting a variety of exercise - alternating between high-impact exercises (e.g. running) and low-impact exercise (e.g. swimming) can help, as it means there are days when the Achilles tendon is under less tension. Limit certain exercises - doing too much hill running, for example, can put excessive strain on the Achilles tendon. Wearing the correct shoes and replacing them when worn - making sure they support the arch and protect the heel will create less tension in the tendon. Using arch supports inside the shoe, if the shoe is in good condition but doesn't provide the required arch support this is a cheaper (and possibly more effective) alternative to replacing the shoe completely. Stretching, doing this before and after exercising helps to keep the Achilles tendon flexible, which means less chance of tendinitis developing. There is no harm in stretching every day (even on days of rest), as this will only further improve flexibility. Gradually increasing the intensity of a workout - Achilles tendinitis can occur when the tendon is suddenly put under too much strain, warming up and increasing the level of activity gradually gives your muscles time to loosen up and puts less pressure on the tendon.
What Triggers Plantar Fasciitis And Approaches To Get Rid Of It
Overview
Plantar fasciitis is a very common condition resulting in pain under the heel which often radiates into the foot. We explain free of charge everything you need to know to cure your pain and prevent it from returning.
Causes
Plantar Fasciitis is caused by abnormal pronation of the foot. Contributing factors are obesity, weight gain, jobs that require a lot of walking or standing on hard surfaces, badly worn shoes with little support, and also inactivity. As a result of over-pronation, with every step the Plantar Fascia (band of tissue under the foot) is being stretched, resulting in inflammation, irritation and pain at the attachment of the fascia into the heel bone. In some cases the pain is felt under the foot, in the arch. Continuous pulling of the fascia at the heel bone, eventually may lead to the development of bony growth on the heel. This is called a heel spur. When you’re at rest, such as while sleeping, the Plantar Fascia tightens and shortens. When body weight is rapidly applied to the foot, the Fascia must stretch and quickly lengthen, causing micro-tears in the Fascia. As a result, the foot pain is more severe with your first steps in the morning, or after sitting for a long period. Plantar Fasciitis is more likely to happen if you suffer from over-pronation (flattening of the arch), you stand or walk on hard surfaces, for long periods, you are overweight or pregnant, you have tight calf muscles.
Symptoms
Plantar fasciitis generally occurs in one foot. Bilateral plantar fasciitis is unusual and tends to be the result of a systemic arthritic condition that is exceptionally rare among athletes. Males suffer from a somewhat greater incidence of plantar fasciitis than females, perhaps as a result of greater weight coupled with greater speed and ground impact, as well as less flexibility in the foot. Typically, the sufferer of plantar fasciitis experiences pain upon rising after sleep, particularly the first step out of bed. Such pain is tightly localized at the bony landmark on the anterior medial tubercle of the calcaneus. In some cases, pain may prevent the athlete from walking in a normal heel-toe gait, causing an irregular walk as means of compensation. Less common areas of pain include the forefoot, Achilles tendon, or subtalar joint. After a brief period of walking, the pain usually subsides, but returns again either with vigorous activity or prolonged standing or walking. On the field, an altered gait or abnormal stride pattern, along with pain during running or jumping activities are tell-tale signs of plantar fasciitis and should be given prompt attention. Further indications of the injury include poor dorsiflexion (lifting the forefoot off the ground) due to a shortened gastroc complex, (muscles of the calf). Crouching in a full squat position with the sole of the foot flat on the ground can be used as a test, as pain will preclude it for the athlete suffering from plantar fasciitis, causing an elevation of the heel due to tension in the gastroc complex.
Diagnosis
Physical examination is the best way to determine if you have plantar fasciitis. Your doctor examines the affected area to determine if plantar fasciitis is the cause of your pain. The doctor may also examine you while you are sitting, standing, and walking. It is important to discuss your daily routine with your doctor. An occupation in which you stand for long periods of time may cause plantar fasciitis. An X-ray may reveal a heel spur. The actual heel spur is not painful. The presence of a heel spur suggests that the plantar fascia has been pulled and stretched excessively for a long period of time, sometimes months or years. If you have plantar fasciitis, you may or may not have a heel spur. Even if your plantar fasciitis becomes less bothersome, the heel spur will remain.
Non Surgical Treatment
Treatment for plantar fasciitis should begin with rest, icing, and over the counter medications. As mentioned above, an orthotic is a device that can be slipped into any pair of shoes and can often relieve pain and help to reverse the damage and occurrence of plantar fasciitis. They do this by adding support to the heel and helping to distribute weight during movement. In addition to orthotics, many people consider night splints for treating this condition. These devices are worn during the night while you sleep, helping to keep the plantar fascia stretched to promote healing. Physical therapy has also become a common option. With this conservative treatment alternative, a physical therapist designs a set of exercises that are intended to address your specific needs in order to promote healing.

Surgical Treatment
Surgery may be considered in very difficult cases. Surgery is usually only advised if your pain has not eased after 12 months despite other treatments. The operation involves separating your plantar fascia from where it connects to the bone; this is called a plantar fascia release. It may also involve removal of a spur on the calcaneum if one is present. Surgery is not always successful. It can cause complications in some people so it should be considered as a last resort. Complications may include infection, increased pain, injury to nearby nerves, or rupture of the plantar fascia.
Stretching Exercises
In one exercise, you lean forward against a wall with one knee straight and heel on the ground. Your other knee is bent. Your heel cord and foot arch stretch as you lean. Hold for 10 seconds, relax and straighten up. Repeat 20 times for each sore heel. It is important to keep the knee fully extended on the side being stretched. In another exercise, you lean forward onto a countertop, spreading your feet apart with one foot in front of the other. Flex your knees and squat down, keeping your heels on the ground as long as possible. Your heel cords and foot arches will stretch as the heels come up in the stretch. Hold for 10 seconds, relax and straighten up. Repeat 20 times. About 90 percent of people with plantar fasciitis improve significantly after two months of initial treatment. You may be advised to use shoes with shock-absorbing soles or fitted with an off-the-shelf shoe insert device like a rubber heel pad. Your foot may be taped into a specific position. If your plantar fasciitis continues after a few months of conservative treatment, your doctor may inject your heel with steroidal anti-inflammatory medication. If you still have symptoms, you may need to wear a walking cast for two to three weeks or a positional splint when you sleep. In a few cases, surgery is needed for chronically contracted tissue.
What Will Cause Painful Heel To Surface

Overview
The Plantar Fascia is a broad, thick band of tissue that runs from under the heel to the front of the foot. Through overuse the fascia can become inflamed and painful at its attachment to the heel bone or calcaneus. The condition is traditionally thought to be inflammation, however this is now believed to be incorrect due to the absence of inflammatory cells within the fascia. The cause of pain is thought to be degeneration of the collagen fibres close to the attachment to the heel bone.
Causes
Plantar fasciitis can develop when your feet roll in too far as you take each step. This rolling in, known as over-pronation, can happen for many reasons. It can be due to excessive weight gain, pregnancy, quickly increasing physical activity, tight calf muscles, poor biomechanics or merely wearing unsupportive, flat footwear. When your feet over-pronate, your arches can collapse, putting strain on the tissues in the bottom of your foot.
Symptoms
The main symptom of plantar fasciitis is heel pain when you walk. You may also feel pain when you stand and possibly even when you are resting. This pain typically occurs first thing in the morning after you get out of bed, when your foot is placed flat on the floor. The pain occurs because you are stretching the plantar fascia. The pain usually lessens with more walking, but you may have it again after periods of rest. You may feel no pain when you are sleeping because the position of your feet during rest allows the fascia to shorten and relax.
Diagnosis
Plantar fasciitis is one of many conditions causing "heel pain". Some other possible causes include nerve compression either in the foot or in the back, stress fracture of the calcaneus, and loss of the fatty tissue pad under the heel. Plantar fasciitis can be distinguished from these and other conditions based on a history and examination done by a physician. It should be noted that heel spurs are often inappropriately thought to be the sole cause of heel pain. In fact, heel spurs are common and are nothing more than the bone's response to traction or pulling-type forces from the plantar fascia and other muscles in the foot where they attach to the heel bone. They are commonly present in patients without pain, and frequently absent from those who have pain. It is the rare patient who has a truly enlarged and problematic spur requiring surgery.
Non Surgical Treatment
Orthotics are corrective foot devices. They are not the same as soft, spongy, rubber footbeds, gel heel cups etc. Gel and rubber footbeds may cushion the heels and feet, but they do not provide any biomechanical correction. In fact, gel can do the opposite and make an incorrect walking pattern even more unstable! Orthotic insoles work by supporting the arches while re-aligning the ankles and lower legs. Most people’s arches look quite normal when sitting or even standing. However, when putting weight on the foot the arches lower, placing added tension on the plantar fascia, leading to inflammation at the heel bone. Orthotics support the arches, which reduces the tension and overwork of the plantar fascia, allowing the inflamed tissue to heal. Orthotics needn’t be expensive, custom-made devices. A comprehensive Heel Pain study by the American Orthopaedic Foot and Ankle Society found that by wearing standard orthotics and doing a number of daily exercises, 95% of patients experienced substantial, lasting relief from their heel pain symptoms.

Surgical Treatment
In cases that do not respond to any conservative treatment, surgical release of the plantar fascia may be considered. Plantar fasciotomy may be performed using open, endoscopic or radiofrequency lesioning techniques. Overall, the success rate of surgical release is 70 to 90 percent in patients with plantar fasciitis. Potential risk factors include flattening of the longitudinal arch and heel hypoesthesia as well as the potential complications associated with rupture of the plantar fascia and complications related to anesthesia.
Prevention
You can help to prevent plantar fasciitis by maintaining a healthy weight, by warming up before participating in sports and by wearing shoes that support the arch and cushion the heel. In people who are prone to episodes of plantar fasciitis, exercises that stretch the heel cord (known as the Achilles tendon) and the plantar fascia may help to prevent plantar fasciitis from returning. Ice massage also can be used on the bottom of the foot after stressful athletic activities. It is possible that strict control of blood sugar will prevent plantar fasciitis in people with diabetes, although this has not been proven.
What Can Cause Heel Discomfort And Ways To Treat It
Overview
The Plantar Fascia is a broad, thick band of tissue that runs from under the heel to the front of the foot. Through overuse the fascia can become inflamed and painful at its attachment to the heel bone or calcaneus. The condition is traditionally thought to be inflammation, however this is now believed to be incorrect due to the absence of inflammatory cells within the fascia. The cause of pain is thought to be degeneration of the collagen fibres close to the attachment to the heel bone.
Causes
Plantar fasciitis is the most common cause of heel pain, accounting for around four out of five cases. Plantar fasciitis is when the thick band of tissue that connects the heel bone with the rest of the foot (the plantar fascia) becomes damaged and thickened. Damage to the plantar fascia is thought to occur following sudden damage, for example, damaging your heel while jogging, running or dancing; this type of damage usually affects younger people who are physically active, gradual wear and tear of the tissues that make up the plantar fascia - this usually affects adults who are 40 years of age or over. You are at an increased risk of gradual wear and tear damaging your plantar fasciitis if you are overweight or obese, if you have a body mass index (BMI) of 30 or over, you are considered to be obese, have a job that involves spending long periods of time standing, wear flat-soled shoes, such as sandals or flip flops. Less common causes of heel pain are a stress fracture. A stress fracture can occur if your heel bone is damaged during an injury. Fat pad atrophy. Fat pad atrophy is where the layer of fat that lies under the heel bone, known as the fat pad, starts to waste away due to too much strain being placed on the pad. Women who wear high-heeled shoes for many years have an increased risk of developing fat pad atrophy. Bursitis. Bursitis is inflammation of one or more bursa (small fluid-filled sacs under the skin, usually found over the joints and between tendons and bones). It's possible to develop bursitis anywhere inside the body, not just in the foot. Tarsal tunnel syndrome. The nerves in the sole of your foot pass through a small tunnel on the inside of the ankle joint, known as the tarsal tunnel. If a cyst forms or the tunnel is damaged, the nerves can become compressed (squashed). This can cause pain anywhere along the nerve, including beneath your heel. Sever's disease. Sever's disease is a common cause of heel pain in children. It's caused by the muscles and tendons of the hamstrings and calves stretching and tightening in response to growth spurts. The stretching of the calf muscle pulls on the Achilles tendon. This pulls on the growing area of bone at the back of the heel (growth plate), causing pain in the heel. The pain is further aggravated by activities such as football and gymnastics. The pain often develops at the side of the heel, but can also be felt under the heel. Calf and hamstring stretches and, if necessary, heel pads are usually effective treatments for Sever's disease. Bone spurs. Bone spurs are an excess growth of bone that forms on a normal bone. Bone spurs can develop on the heel (a heel spur) and are more common in people with heel pain. However, they can also occur in people without heel pain. A heel spur does not cause heel pain.
Symptoms
The symptoms of plantar fasciitis include pain in the bottom of your foot, especially at the front or centre of the heel bone, pain that is worse when first rising in the morning (called "first-step pain"), when first standing up after any long period of sitting, or after increased levels of activity especially in non-supportive shoes. Seek medical advice about plantar fasciitis if you have heel pain or pain in the bottom of your foot, especially when you get up in the morning, that does not respond to treatment or if there is redness or bruising in the heel.
Diagnosis
Most cases of plantar fasciitis are diagnosed by a health care provider who listens carefully to your description of symptoms. During an examination of your feet, your health care provider will have to press on the bottom of your feet, the area most likely to be painful in plantar fasciitis. Because the pain of plantar fasciitis has unique characteristics, pain upon rising, improvement after walking for several minutes, pain produced by pressure applied in a specific location on your foot but not with pressure in other areas, your health care provider will probably feel comfortable making the diagnosis based on your symptoms and a physical examination. Your health care provider may suggest that you have an X-ray of your foot to verify that there is no stress fracture causing your pain.
Non Surgical Treatment
The following self-help treatments have been found to be most effective. Rest your foot. Reduce the amount of weight-bearing activities you participate in. Get off of your feet and elevate them. This will allow healing to begin. Apply ice to your foot. Applications of ice packs that provide a comfortable cooling to the heel and arch (not a freezing cold) will help reduce pain, swelling, and inflammation. Apply the ice to the heel and arch (not the toes). Make sure it is comfortable, and leave on your foot for about 20 minutes, 3 times a day. If you have any medical problems such as diabetes, poor circulation, etc., discuss the use of ice with your doctor before applying the ice. ActiveWrap allows you to apply comfortable cold therapy to your foot without messy ice cubes. Use while on the "go." Do not walk with bare feet. Always protect your heels, arches, and plantar fascia with good supportive shoes. Orthaheel Orthotic Flip Flops For Men and Women are designed for walking comfort with built in orthotic footbeds that help reduce foot pain from plantar fasciitis. Use in the house or on the beach. Stretch the Plantar Fascia while sleeping. Plantar Fasciitis and Heel Spur pain is usually worse with the first steps in the morning. This is due to the Plantar Fascia tightening up, or contracting while we sleep. To prevent these pain producing contractures of the plantar fascia, the foot must be held in its normal or neutral position while we sleep. This optimal position of the foot is maintained with our comfortable and supportive Night Splint. When foot contractures are prevented during sleep, the "first step pains" Plantar Fasciitis and Heel Spurs will gradually subside. Stretch the Plantar Fascia during the day. Even though the Plantar Fascia is a thick tissue band with very little "give" to it, with the proper care (a Night Splint and the following exercises) it can be stretched a small amount. By stretching the Plantar Fascia even a bit, its abnormal pull on the heel is reduced. This will help to reduce pain and inflammation in the heel and arch. Two of the most effective exercises recommended are. Before stepping down, especially after sleeping or resting, stretch the arch of the foot by stretching your legs out in front of you (do not bend the knee). Place a towel around the ball of the foot. Slowly pull on the ends of the towel, pulling the toes and ball of the foot back as far as is comfortable. Hold the foot in this position for ten seconds. Repeat at least ten times. You should feel a pull on the bottom of the foot, especially in the arch. This stretches the plantar fascia, and reduces its pull on the heel. Stand about 2 to 3 feet from a wall. Lean forward with your hands against the wall. With the painful foot behind, place the other foot forward. Press against the wall, shifting weight over the front foot, while straightening the back leg. Keep the heel of the back foot on the floor and feel the stretch in the heel, Achilles tendon, and calf. Hold this position for ten seconds. Repeat at least ten times, and try to do this three times a day. When these things are achieved, the inflammation and pain of Plantar Fasciitis and Heel Spurs will gradually subside. If you are unsure of the nature of your foot problem, if your pain is intense and does not subside, if you are a diabetic or have other medical problems, if your pain is due to an injury, if an open sore is present, if a mass can be felt, or if you think that you may have an infection, we suggest that before beginning any of the above treatments you consult with your doctor.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints, a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as, open surgery, where the section of the plantar fascia is released by making a cut into your heel, endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team. Extracorporeal shockwave therapy (EST) is a fairly new type of non-invasive treatment. Non-invasive means it does not involve making cuts into your body. EST involves using a device to deliver high-energy soundwaves into your heel. The soundwaves can sometimes cause pain, so a local anaesthetic may be used to numb your heel. It is claimed that EST works in two ways. It is thought to, have a "numbing" effect on the nerves that transmit pain signals to your brain, help stimulate and speed up the healing process. However, these claims have not yet been definitively proven. The National Institute for Health and Care Excellence (NICE) has issued guidance about the use of EST for treating plantar fasciitis. NICE states there are no concerns over the safety of EST, but there are uncertainties about how effective the procedure is for treating heel pain. Some studies have reported that EST is more effective than surgery and other non-surgical treatments, while other studies found the procedure to be no better than a placebo (sham treatment).
Prevention
The following steps will help prevent plantar fasciitis or help keep the condition from getting worse if you already have it. Take care of your feet. Wear shoes with good arch support and heel cushioning. If your work requires you to stand on hard surfaces, stand on a thick rubber mat to reduce stress on your feet. Do exercises to stretch the Achilles tendon at the back of the heel. This is especially important before sports, but it is helpful for non-athletes as well. Ask your doctor about recommendations for a stretching routine. Stay at a healthy weight for your height. Establish good exercise habits. Increase your exercise levels gradually, and wear supportive shoes. If you run, alternate running with other sports that will not cause heel pain. Put on supportive shoes as soon as you get out of bed. Going barefoot or wearing slippers puts stress on your feet. If you feel that work activities caused your heel pain, ask your human resources department for information about different ways of doing your job that will not make your heel pain worse. If you are involved in sports, you may want to consult a sports training specialist for training and conditioning programs to prevent plantar fasciitis from recurring.